Update on Ebola Bundibugyo Outbreak
Introduction
This brief summarizes the current Ebola Bundibugyo outbreak in eastern Democratic Republic of the Congo (DRC) and Uganda. On May 17, the World Health Organization declared the outbreak a Public Health Emergency of International Concern, underscoring the seriousness of the event and the need for coordinated national, regional, and international response. The brief brings together official public health reporting, humanitarian situation updates, and contextual analysis to highlight the outbreak chronology, epidemiology, treatment and vaccine status, movement and travel measures, and the social, cultural, mobility, and conflict factors likely to shape response operations.
[Source: Center for Disease Prevention and Control (CDC). Ebola Outbreak: Current Situation, 2026. Retrieved from https://www.cdc.gov/ebola/situation-summary/index.html]
Executive summary
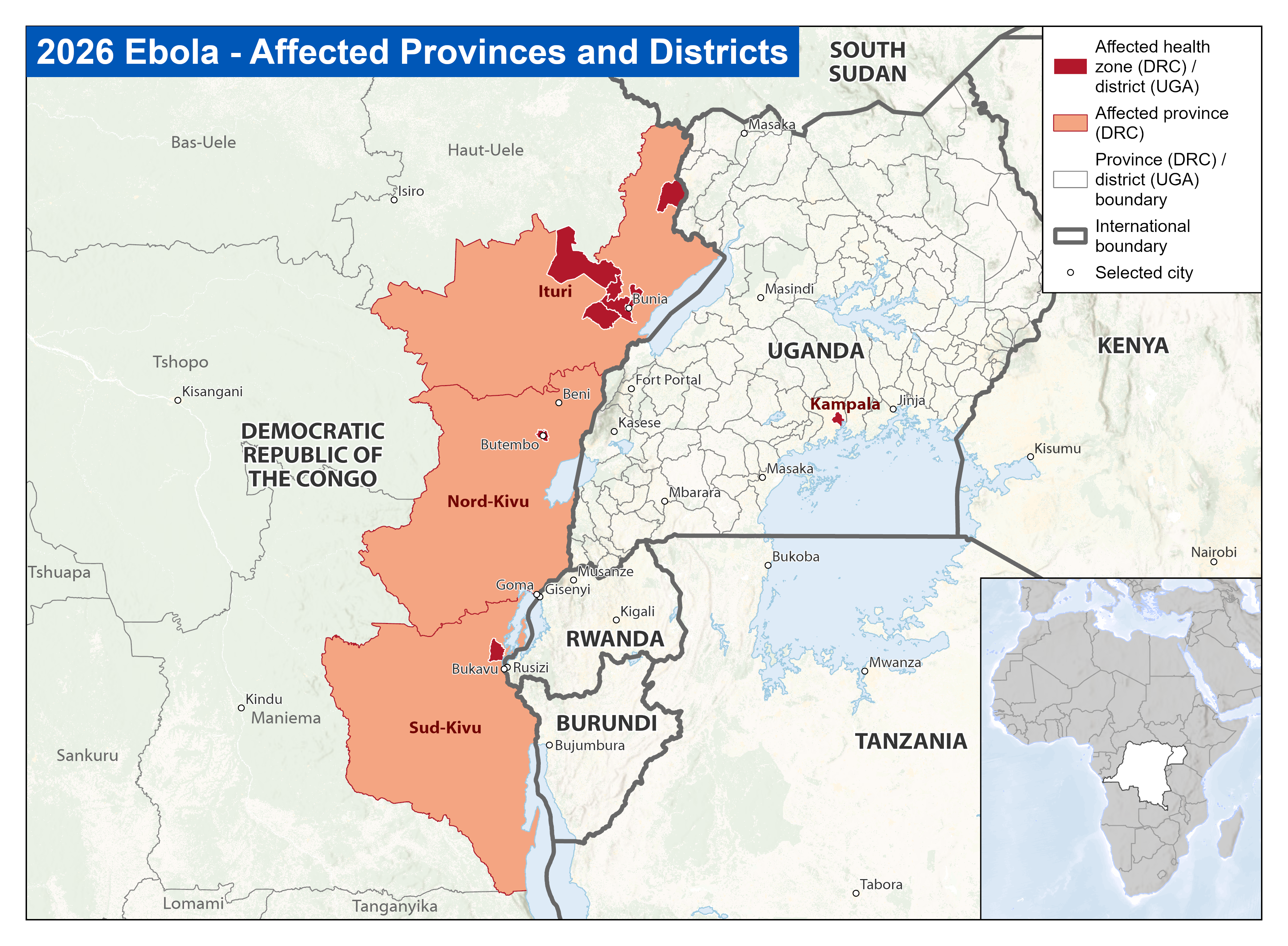
The Ebola outbreak caused by Bundibugyo virus disease (BVD) is affecting the Democratic Republic of the Congo (DRC) and Uganda, with confirmed DRC cases in Ituri, Nord-Kivu, and Sud-Kivu provinces and Uganda cases linked to the DRC outbreak. In the latest reporting on 5 June, the DRC Ministry of Health reported 381 confirmed Bundibugyo virus disease cases and 64 confirmed deaths as of 3 June, with Ituri remaining the most affected province. As of 5 June, Uganda had reported 19 confirmed cases and two deaths, bringing the combined total across DRC and Uganda to 400 confirmed cases and 66 confirmed deaths—an increase of 266 confirmed cases and 48 confirmed deaths since the 29 May WHO update. CDC states that no outbreak-associated Ebola cases have been confirmed in the United States and that risk to the U.S. public and travelers remains low. [1]
The outbreak is unfolding in a highly complex operating environment: Ituri has roughly 5.9-7 million inhabitants, nearly 1 million displaced people, major ethnic and linguistic diversity, high mobility linked to mining and trade, and persistent insecurity involving armed groups, roadblocks, displacement, and attacks on health infrastructure. The response must therefore address not only virology and case management, but also contextual local factors such as trust, burial practices, informal care pathways, displacement, cross-border movement, and conflict-sensitive access. [12-14]
Chronology and timing of key events
The earliest publicly reported exposure cluster is not a confirmed index case, but it suggests that transmission may have preceded formal detection by several weeks. The International Federation of Red Cross and Red Crescent Societies (IFRC) reported that three DRC Red Cross volunteers from the Mongbwalu branch in Djugu Territory were believed to have contracted Ebola while conducting dead body management on 27 March 2026, before the outbreak was known to be Ebola. This should be described as the earliest publicly reported exposure cluster, not the index case, because infection during body management implies a preceding infected deceased person or transmission chain. [6]
DRC official situation reporting indicates that a preliminary health signal arose on 5 May 2026 from health personnel in Mongbwalu Health Zone and was officially notified on 8 May, following reports of grouped unexplained deaths, including reports of approximately 50 deaths circulating through social media. Between 1 April and 13 May, DRC reporting described hundreds of suspected or probable cases and about 100 deaths in the Mongbwalu area, including deaths among health professionals. [8]
On May 14 , investigations and laboratory testing accelerated. Initial testing was negative for Ebola Zaire and several other pathogens, but INRB Kinshasa later tested 13 samples, with 8 positives for non-Zaire Ebola virus. On 15 May, sequencing identified the strain as Bundibugyo, enabling the DRC Minister of Public Health, Hygiene and Social Welfare to officially declare the country's 17th Ebola outbreak. [3,7]
After confirmation, case counts rose rapidly and the outbreak expanded geographically. DRC situation reports by 19-23 May documented affected health zones in Ituri and Nord-Kivu, later including Sud-Kivu. As of 27 May, the DRC had reported 906 suspected cases and 223 deaths among suspected cases. By 29 May, 134 confirmed cases, including nine in Uganda, and 18 confirmed deaths had been reported across both countries, representing an increase of 49 confirmed cases, eight confirmed deaths, 160 suspected cases, and 47 suspected deaths since 21 May. A tripartite DRC-Uganda-South Sudan coordination meeting took place in Kampala on 23 May to harmonize surveillance, alert notification, suspected case management, and cross-border contact follow-up at points of entry and control. [9-11]
Context: location, culture, mobility, and conflict
The outbreak is unfolding primarily in eastern DRC, especially Ituri Province, with confirmed spread into Nord-Kivu and Sud-Kivu. Ituri has an estimated 5.9-7 million people, including nearly 1 million internally displaced persons, and includes urban centres such as Bunia, important mining areas such as Mongbwalu, and multiple administrative and health-zone boundaries that do not always align. The province is socially and linguistically diverse, with major groups including Hema, Lendu, Alur, Lugbara, and Nande. Swahili and Lingala are widely used, French is mainly used by elites, and local languages such as Lendu and Nyali are important in rural and displaced communities. Response communication therefore needs to be locally translated, tested, and adapted to different audiences, particularly because biomedical vocabulary may not be well understood in common lingua francas. [12]
The conflict environment is a central feature of the outbreak context. Insecurity in Ituri should not be understood simply as an ethnic conflict between Hema and Lendu communities. It is rooted in long-standing disputes over land, political authority, exclusion, elite manipulation, gold-linked economic interests, and armed control of mobility, taxation, and access. Since 2017, renewed violence has generated large-scale displacement, particularly in Djugu territory, where CODECO/URDPC and Zaire armed-group dynamics have made humanitarian access unpredictable. ADF violence in Irumu and Mambasa, including attacks on civilians, health facilities, and road users, further constrains surveillance, referral, sample transport, contact tracing, and response-team safety. Roadblocks and checkpoints turn movement into a site of extortion and negotiation, complicating access to affected communities and movement along trade, mining, displacement, and care-seeking routes. [12,14]
Mobility is central to outbreak risk. Artisanal gold mining structures the provincial economy and generates major population movement to sites such as Mongbwalu. Mining sites are not socially unstructured spaces; they include pit bosses, traders, transporters, young male workers, food sellers, service providers, and other actors who should be engaged in surveillance, risk communication, and referral. Ituri is also highly connected to Uganda and South Sudan through formal and informal routes, while Nord-Kivu links to Uganda and Rwanda. Cross-border trade, displacement, family networks, transport corridors, and mining-related mobility increase the risk of undetected transmission and complicate contact tracing. [12,13]
The social and cultural context has direct implications for control measures. Religious institutions, especially Catholic, Protestant, and revival churches, play important roles in health, education, local authority, and community trust. Religious leaders can strongly influence acceptance of care, safe burial, surveillance, vaccination or trial messaging, and broader response legitimacy. Funeral practices are also a major transmission and trust issue: body washing, touching, mourning gatherings, transport of bodies, prayers, family presence, and burial location are socially and spiritually significant. Safe and dignified burial should therefore adapt rituals rather than simply prohibit them. Family consultation, prayers, photographs or videos where acceptable, family escort, and safe ritual substitutes may help avoid clandestine burials and community resistance. [12,14]
Epidemiology, clinical features, treatment, and vaccine status
Bundibugyo virus disease is a severe form of Ebola disease. WHO describes transmission as occurring through direct contact with blood, secretions, organs, or other bodily fluids of infected or deceased people, or through contaminated surfaces and materials. Transmission is amplified when infection prevention and control is inadequate in health-care settings and during unsafe burial practices. The incubation period ranges from 2 to 21 days, and people are usually not infectious until symptoms appear. [3,5]
CDC reports that patients in this outbreak have experienced symptoms including fever, headache, vomiting, severe weakness, abdominal pain, nosebleeds, and vomiting blood. CDC also notes that most DRC cases reported to date have been among people aged 20-39 years, with approximately two-thirds among female patients. [1]
There is currently no licensed or approved vaccine for Bundibugyo virus disease, and there is no FDA-approved or authorized treatment specifically for BVD. The U.S.-licensed Ebola vaccine ERVEBO is indicated for prevention of disease caused by Zaire ebolavirus and is not expected to protect against Bundibugyo virus. Treatment therefore remains based on early, high-quality supportive care, including oral and intravenous rehydration, electrolyte management, fever and pain control, treatment of bacterial superinfections or other complications, nutritional support, and careful clinical monitoring. [1-3,5]
However, no licensed vaccine does not mean there is no vaccine research. The University of Oxford has announced that the Oxford Vaccine Group, working with Oxford's Clinical BioManufacturing Facility and the Serum Institute of India, is urgently producing and scaling doses of a ChAdOx-based monovalent Bundibugyo ebolavirus candidate vaccine, ChAdOx1 BDBV. This candidate remains investigational: Oxford states that it is accelerating the generation of supportive preclinical data for clinical development and testing, while following scientific, ethical, and regulatory standards. WHO similarly notes that there is currently no vaccine or specific treatment for Bundibugyo virus disease, although work is ongoing to test promising candidates. For the present response, supportive care, early detection, isolation, IPC, contact tracing, safe and dignified burial, and community engagement remain the core control measures while vaccine candidates undergo further research. [5,17]
International Response: movement, border, and travel restriction status
Movement controls, border screening, and point-of-entry measures are evolving rapidly across the affected region. ACAPS reported that Uganda had begun restricting movement across the Ishasha-Kyeshero border crossing, that some people attempting to cross into Rwanda from Goma and Bukavu had been stopped, and that South Sudan had issued an alert and begun monitoring its border with DRC. These measures may help reduce onward transmission, but they also risk disrupting trade, livelihoods, education, humanitarian access, and access to essential services, particularly for border communities that depend on daily mobility. [14]
IOM is supporting a mobility-informed response across points of entry, points of control, and high-mobility corridors. In DRC, IOM reports support for PoE and PoC operations in Bunia, Beni, Goma, and N'djili International Airport, including activation of five points of control at key exits from Bunia, mapping of formal and informal crossings along the Uganda border, and analysis of direct and indirect air routes linked to Bunia, Kisangani, Isiro, Beni, Kalemie, Aru, and mining-site airstrips. In Uganda, IOM is conducting flow monitoring across 12 points of entry, including seven sites along the DRC border, and is supporting health screening at border points and airports. IOM is also supporting preparedness, surveillance, RCCE, IPC/WASH, and PoE activities in South Sudan, Burundi, Rwanda, Angola, Central African Republic, Ethiopia, Kenya, and Tanzania. WHO has identified DRC, Uganda, South Sudan, Burundi, and Rwanda as Priority 1 countries for readiness and response, with Angola, Central African Republic, Ethiopia, Kenya, Republic of Congo, Tanzania, and Zambia identified as Priority 2 countries. [13]
For the United States, the Centers for Disease Control and Prevention (CDC) and the Department of Homeland Security (DHS) announced enhanced travel screening, entry restrictions, and public health measures on 18 May 2026 to reduce the risk of Ebola entering the country. CDC states that travelers who were in DRC, Uganda, or South Sudan during the 21 days before arrival to the United States may be subject to enhanced public health screening and monitoring. Certain non-U.S. citizens who were recently in DRC, Uganda, or South Sudan are temporarily restricted from entering the United States. U.S. citizens and nationals may still enter, but they will undergo enhanced public health screening and should monitor for Ebola symptoms for 21 days after leaving the affected countries. [1,18]
CDC indicates that affected travelers may be rerouted to selected U.S. airports, including Washington-Dulles International Airport, Hartsfield-Jackson Atlanta International Airport, and George Bush Intercontinental Airport in Houston, where screening includes travel history, symptom assessment, temperature checks, and collection of contact information for follow-up if needed. CDC Travel Health Notices identify DRC as experiencing Bundibugyo virus disease in Ituri, Nord-Kivu, and Sud-Kivu provinces and Uganda as experiencing linked cases. CDC states that no Ebola cases associated with this outbreak have been confirmed in the United States and that the risk to the U.S. public remains low. [1,18,19]
Latest information Sources
The World Health Organization
https://www.who.int/emergencies/disease-outbreak-news/item/2026-DON605
The World Health Organization African Region (WHO AFRO)
Africa Centres for Disease Control and Prevention (Africa CDC)
https://africacdc.org/about-us/
United States Centers for Disease Control and Prevention (CDC)
https://www.cdc.gov/ebola/situation-summary/index.html
Ministry of Public Health, Hygiene and Social Security of the Democratic Republic of the Congo Official Dashboard:
https://sante.gouv.cd/epidemie/ebola-bundibugyo-2026#
Institute of Public Health Dashboard
[1] Centers for Disease Control and Prevention (CDC). Ebola Disease: Current Situation. Updated 27 May 2026. https://www.cdc.gov/ebola/situation-summary/index.html
[2] CDC Health Alert Network. Ebola Disease Outbreak in the Democratic Republic of the Congo and Uganda, HAN 00530. 2026. https://www.cdc.gov/han/php/notices/han00530.html
[3] World Health Organization (WHO). Disease Outbreak News DON602: Ebola disease caused by Bundibugyo virus - Democratic Republic of the Congo and Uganda. 16 May 2026. https://www.who.int/emergencies/disease-outbreak-news/item/2026-DON602
[4] World Health Organization (WHO). Disease Outbreak News DON603: Ebola disease caused by Bundibugyo virus - Democratic Republic of the Congo and Uganda. 21 May 2026. https://www.who.int/emergencies/disease-outbreak-news/item/2026-DON603
[5] World Health Organization (WHO). Ebola outbreak - DRC 2026 situation page. https://www.who.int/emergencies/situations/ebola-outbreak---drc-2026
[6] International Federation of Red Cross and Red Crescent Societies (IFRC). Statement: IFRC saddened by deaths of three DRC Red Cross volunteers in Ituri Province. 23 May 2026. https://www.ifrc.org/article/statement-ifrc-saddened-deaths-three-drc-red-cross-volunteers-ituri-province
[7] Ministere de la Sante Publique, Hygiene et Prevoyance Sociale, DRC. Declaration de la 17e epidemie de maladie a virus Ebola dans les zones de sante de Rwampara, Mongwalu et Bunia. 15 May 2026. https://administration.sante.gouv.cd/wp-content/uploads/2026/05/Declaration-de-la-17e-Epidemie-de-la-maladie-a-virus-Ebola-dans-les-zones-de-sante-de-Rwampara-Mongwalu-et-Bunia-dans-la-province-dIturi.pdf
[8] INSP/COUSP-RDC. SitRep MVE Ituri No. 001/2026, reporting date 14 May 2026, publication 15 May 2026. https://insp.cd/wp-content/uploads/2026/05/Draft-MVE-Ituri-ActuelB-1.pdf
[9] INSP/COUSP-RDC. SitRep MVE RDC No. 005/2026, reporting date 19 May 2026. https://insp.cd/wp-content/uploads/2026/05/Draft_SitRep_MVE_RDC_20260520_vf1.pdf
[10] INSP/COUSP-RDC. SitRep MVE RDC No. 009/MVB_24/2026, reporting date 23 May 2026, publication 24 May 2026. https://insp.cd/wp-content/uploads/2026/05/SitRep_MVE_RDC_2024fv1_IM.pdf
[11] Ministere de la Sante Publique, Hygiene et Prevoyance Sociale, DRC. Ebola Bundibugyo: regional coordination strengthened in Kampala. 2026. https://sante.gouv.cd/actualites/ebola-bundibugyo-la-rdc-louganda-et-le-soudan-du-sud-scellent-une-coordination-regionale-renforcee-a-kampala
[12] Villa J, Amuda DM, Araali B, et al. Contextual Note on the Ebola Bundibugyo Outbreak in Ituri (2026). HAL Open Science. 26 May 2026. https://hal.science/hal-05632368v1
[13] International Organization for Migration (IOM). Multi-Country Ebola Bundibugyo Outbreak Situation Report No. 1, 15-21 May 2026. ReliefWeb. https://reliefweb.int/report/democratic-republic-congo/iom-multi-country-ebola-bundibugyo-outbreak-situation-report-no-1-15-21-may-2026
[14] ACAPS. Briefing Note: DRC Ebola outbreak. 22 May 2026. https://reliefweb.int/report/democratic-republic-congo/acaps-briefing-note-drc-ebola-outbreak-22-may-2026
[15] UNFPA. Flash Update on the Ebola Outbreak in DRC, 14-19 May 2026. https://www.unfpa.org/resources/unfpa-flash-update-ebola-outbreak-drc-14-19-may-2026
[16] International Medical Corps. Ebola Outbreak in the DRC and Region: What You Need to Know. 22 May 2026. https://internationalmedicalcorps.org/story/ebola-outbreak-in-the-drc-and-region-what-you-need-to-know/
[17] University of Oxford. Statement on vaccine efforts relating to the Bundibugyo Ebolavirus outbreak in the DRC. 22 May 2026. https://www.ox.ac.uk/news/2026-05-22-statement-on-vaccine-efforts-relating-to-the-bundibugyo-ebolavirus-outbreak-in-the
[18] CDC. What Travelers Need to Know About Returning to the United States from DRC, Uganda, and South Sudan. Updated 23 May 2026. https://www.cdc.gov/viral-hemorrhagic-fevers/travel-to-us/index.html
[19] CDC Travelers Health. Travel Health Notices. https://wwwnc.cdc.gov/travel/notices